
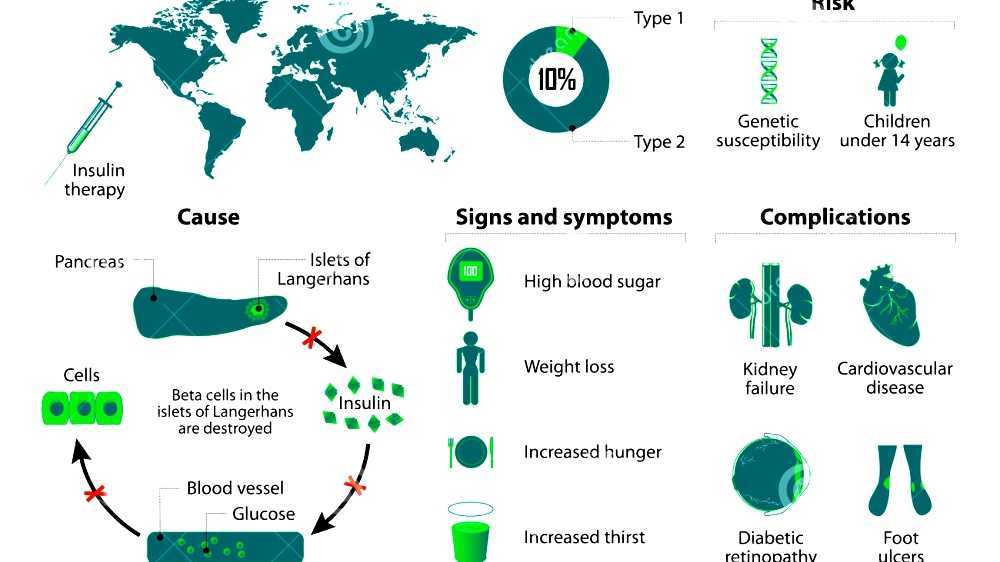

Diabetes mellitus type 1 (also known as type 1 diabetes) is a form of diabetes mellitus in which not enough insulin is produced. This results in high blood sugar levels in the body. The classical symptoms are frequent urination, increased thirst, increased hunger, and weight loss. Additional symptoms may include blurry vision, feeling tired, and poor healing. Symptoms typically develop over a short period of time.
The cause of type 1 diabetes is unknown. However, it is believed to involve a combination of genetic and environmental factors. Risk factors include having a family member with the condition. The underlying mechanism involves an autoimmune destruction of the insulin-producing beta cells in the pancreas. Diabetes is diagnosed by testing the level of sugar or A1C in the blood. Type 1 diabetes can be distinguished from type 2 by testing for the presence of autoantibodies.
There is no known way to prevent type 1 diabetes. Treatment with insulin is required for survival. Insulin therapy is usually given by injection just under the skin but can also be delivered by an insulin pump. A diabetic diet and exercise are an important part of management. Untreated, diabetes can cause many complications. Complications of relatively rapid onset include diabetic ketoacidosis and nonketotic hyperosmolar coma. Long-term complications include heart disease, stroke, kidney failure, foot ulcers and damage to the eyes. Furthermore, complications may arise from low blood sugar caused by excessive dosing of insulin.
Type 1 diabetes makes up an estimated 5-10% of all diabetes cases. The number of people affected globally is unknown, although it is estimated that about 80,000 children develop the disease each year. Within the United States the number of people affected is estimated at one to three million. Rates of disease vary widely with approximately 1 new case per 100,000 per year in East Asia and Latin America and around 30 new cases per 100,000 per year in Scandinavia and Kuwait. It typically begins in children and young adults.
Video Diabetes mellitus type 1
Signs and symptoms
The classical symptoms of type 1 diabetes include: polyuria (excessive urination), polydipsia (increased thirst), dry mouth, polyphagia (increased hunger), fatigue, and weight loss.
Many type 1 diabetics are diagnosed when they present with diabetic ketoacidosis. The signs and symptoms of diabetic ketoacidosis include dry skin, rapid deep breathing, drowsiness, increased thirst, frequent urination, abdominal pain, and vomiting.
About 12 percent of people with type 1 diabetes have clinical depression.
About 6 percent of people with type 1 diabetes have celiac disease, but in most cases there are no digestive symptoms or are mistakenly attributed to poor control of diabetes, gastroparesis or diabetic neuropathy. In most cases, celiac disease is diagnosed after onset of type 1 diabetes. The association of celiac disease with type 1 diabetes increases the risk of complications, such as retinopathy and mortality. This association can be explained by shared genetic factors, and inflammation or nutritional deficiencies caused by untreated celiac disease, even if type 1 diabetes is diagnosed first.
Some people with type 1 diabetes experience dramatic and recurrent swings in glucose levels, often occurring for no apparent reason; this is called "unstable diabetes" or "labile diabetes", and sometimes "brittle diabetes", although this term is no longer used. The results of such swings can be irregular and unpredictable hyperglycemias, sometimes involving ketoacidosis, and sometimes serious hypoglycemias. Brittle diabetes occurs no more frequently than in 1% to 2% of diabetics.
Maps Diabetes mellitus type 1
Cause
The cause of type 1 diabetes is unknown. A number of explanatory theories have been put forward, and the cause may be one or more of the following: genetic susceptibility, a diabetogenic trigger, and exposure to an antigen.
Genetics
Type 1 diabetes is a disease that involves many genes. The risk of a child developing type 1 diabetes is about 5% if the father has it, about 8% if a sibling has it, and about 3% if the mother has it. If one identical twin is affected there is about a 50% chance the other will also be affected. Some studies of heritability has estimated it at 80 to 86%.
More than 50 genes are associated with type 1 diabetes. Depending on locus or combination of loci, they can be dominant, recessive, or somewhere in between. The strongest gene, IDDM1, is located in the MHC Class II region on chromosome 6, at staining region 6p21. Certain variants of this gene increase the risk for decreased histocompatibility characteristic of type 1. Such variants include DRB1 0401, DRB1 0402, DRB1 0405, DQA 0301, DQB1 0302 and DQB1 0201, which are common in North Americans of European ancestry and in Europeans. Some variants also appear to be protective.
Environmental
Environmental factors can influence expression of type 1. For identical twins, when one twin has type 1 diabetes, the other twin only has it 30%-50% of the time. Thus for 50%-70% of identical twins where one has the disease, the other will not, despite having exactly the same genome; this suggests that environmental factors, in addition to genetic factors, can influence the disease's prevalence. Other indications of environmental influence include the presence of a 10-fold difference in occurrence among Caucasians living in different areas of Europe, and that people tend to acquire the rate of disease of their particular destination country. Research is ongoing into the role of possible environmental triggers and protective factors, including dietary agents such as proteins in gluten, time of weaning, gut microbiota and viral infections.
Chemicals and drugs
Some chemicals and drugs selectively destroy pancreatic cells. Pyrinuron (Vacor), a rodenticide introduced in the United States in 1976, selectively destroys pancreatic beta cells, resulting in type 1 diabetes after accidental poisoning. Pyrinuron was withdrawn from the U.S. market in 1979 and it is not approved by the Environmental Protection Agency for use in the U.S. Streptozotocin (Zanosar), an antineoplastic agent, is selectively toxic to the beta cells of the pancreatic islets. It is used in research for inducing type 1 diabetes on rodents and for treating metastatic cancer of the pancreatic islet cells in patients whose cancer cannot be removed by surgery. Other pancreatic problems, including trauma, pancreatitis, or tumors (either malignant or benign) can also lead to loss of insulin production.

Pathophysiology
The pathophysiology in diabetes type 1 is a destruction of beta cells in the pancreas, regardless of which risk factors or causative entities have been present.
Individual risk factors can have separate pathophysiological processes to, in turn, cause this beta cell destruction. Still, a process that appears to be common to most risk factors is an autoimmune response towards beta cells, involving an expansion of autoreactive CD4+ T helper cells and CD8+ T cells, autoantibody-producing B cells and activation of the innate immune system.
After starting treatment with insulin a person's own insulin levels may temporarily improve. This is believed to be due to altered immunity and is known as the "honeymoon phase".

Diagnosis
Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by demonstrating any one of the following:
- Fasting plasma glucose level at or above 7.0 mmol/L (126 mg/dL).
- Plasma glucose at or above 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose load as in a glucose tolerance test.
- Symptoms of hyperglycemia and casual plasma glucose at or above 11.1 mmol/L (200 mg/dL).
- Glycated hemoglobin (hemoglobin A1C) at or above 48 mmol/mol (>= 6.5 DCCT %). (This criterion was recommended by the American Diabetes Association in 2010, although it has yet to be adopted by the WHO.)
About a quarter of people with new type 1 diabetes have developed some degree of diabetic ketoacidosis (a type of metabolic acidosis which is caused by high concentrations of ketone bodies, formed by the breakdown of fatty acids and the deamination of amino acids) by the time the diabetes is recognized. The diagnosis of other types of diabetes is usually made in other ways. These include ordinary health screening, detection of hyperglycemia during other medical investigations, and secondary symptoms such as vision changes or unexplained fatigue. Diabetes is often detected when a person suffers a problem that may be caused by diabetes, such as a heart attack, stroke, neuropathy, poor wound healing or a foot ulcer, certain eye problems, certain fungal infections, or delivering a baby with macrosomia or hypoglycemia (low blood sugar).
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. Most physicians prefer to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test. According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
In type 1, pancreatic beta cells in the islets of Langerhans are destroyed, decreasing endogenous insulin production. This distinguishes type 1's origin from type 2. Type 2 diabetes is characterized by insulin resistance, while type 1 diabetes is characterized by insulin deficiency, generally without insulin resistance. Another hallmark of type 1 diabetes is islet autoreactivity, which is generally measured by the presence of autoantibodies directed towards the beta cells.
Autoantibodies
The appearance of diabetes-related autoantibodies has been shown to be able to predict the appearance of diabetes type 1 before any hyperglycemia arises, the main ones being islet cell autoantibodies, insulin autoantibodies, autoantibodies targeting the 65-kDa isoform of glutamic acid decarboxylase (GAD), autoantibodies targeting the phosphatase-related IA-2 molecule, and zinc transporter autoantibodies (ZnT8). By definition, the diagnosis of diabetes type 1 can be made first at the appearance of clinical symptoms and/or signs, but the emergence of autoantibodies may itself be termed "latent autoimmune diabetes". Not everyone with autoantibodies progresses to diabetes type 1, but the risk increases with the number of antibody types, with three to four antibody types giving a risk of progressing to diabetes type 1 of 60%-100%. The time interval from emergence of autoantibodies to clinically diagnosable diabetes can be a few months in infants and young children, but in some people it may take years - in some cases more than 10 years. Islet cell autoantibodies are detected by conventional immunofluorescence, while the rest are measured with specific radiobinding assays.

Prevention
Type 1 diabetes is not currently preventable. Some researchers believe it might be prevented at the latent autoimmune stage, before it starts destroying beta cells.
Immunosuppressive drugs
Cyclosporine A, an immunosuppressive agent, has apparently halted destruction of beta cells (on the basis of reduced insulin usage), but its kidney toxicity and other side effects make it highly inappropriate for long-term use.
Anti-CD3 antibodies, including teplizumab and otelixizumab, had suggested evidence of preserving insulin production (as evidenced by sustained C-peptide production) in newly diagnosed type 1 diabetes patients. A probable mechanism of this effect was believed to be preservation of regulatory T cells that suppress activation of the immune system and thereby maintain immune system homeostasis and tolerance to self-antigens. The duration of the effect is still unknown, however. In 2011, Phase III studies with otelixizumab and teplizumab both failed to show clinical efficacy, potentially due to an insufficient dosing schedule.
An anti-CD20 antibody, rituximab, inhibits B cells and has been shown to provoke C-peptide responses three months after diagnosis of type 1 diabetes, but long-term effects of this have not been reported.
Diet
Some research has suggested breastfeeding decreases the risk in later life and early introduction of gluten-containing cereals in the diet increases the risk of developing islet cell autoantibodies; various other nutritional risk factors are being studied, but no firm evidence has been found. Giving children 2000 IU of vitamin D daily during their first year of life is associated with reduced risk of type 1 diabetes, though the causal relationship is obscure.
Children with antibodies to beta cell proteins (i.e. at early stages of an immune reaction to them) but no overt diabetes, and treated with niacinamide (vitamin B3), had less than half the diabetes onset incidence in a seven-year time span than did the general population, and an even lower incidence relative to those with antibodies as above, but who received no niacinamide.
People with type 1 diabetes and undiagnosed celiac disease have worse glycaemic control and a higher prevalence of nephropathy and retinopathy. Gluten-free diet, when performed strictly, improves diabetes symptoms and appears to have a protective effect against developing long-term complications. Nevertheless, dietary management of both these diseases is challenging and these patients have poor compliance of the diet.

Management
Diabetes is often managed by a number of health care providers including a dietitian, nurse educator, eye doctor, endocrinologist, and podiatrist.
Lifestyle
A low-carbohydrate diet, exercise, and medications is useful in type 1 DM. There are camps for children to teach them how and when to use or monitor their insulin without parental help. As psychological stress may have a negative effect on diabetes, a number of measures have been recommended including: exercising, taking up a new hobby, or joining a charity among others.
Insulin
Injections of insulin--either via subcutaneous injection or insulin pump-- are necessary for those living with type 1 diabetes because it cannot be treated by diet and exercise alone. Insulin dosage is adjusted taking into account food intake, blood glucose levels and physical activity.
Untreated type 1 diabetes can commonly lead to diabetic ketoacidosis which is a diabetic coma which can be fatal if untreated. Diabetic ketoacidosis can cause cerebral edema (accumulation of liquid in the brain). This is a life-threatening issue and children are at a higher risk for cerebral edema than adults, causing ketoacidosis to be the most common cause of death in pediatric diabetes.
Treatment of diabetes focuses on lowering blood sugar or glucose (BG) to the near normal range, approximately 80-140 mg/dl (4.4-7.8 mmol/L). The ultimate goal of normalizing BG is to avoid long-term complications that affect the nervous system (e.g. peripheral neuropathy leading to pain and/or loss of feeling in the extremities), and the cardiovascular system (e.g. heart attacks, vision loss). This level of control over a prolonged period of time can be varied by a target HbA1c level of less than 7.5%.
There are four main types of insulin: rapid acting insulin, short-acting insulin, intermediate-acting insulin, and long-acting insulin. The rapid acting insulin is used as a bolus dosage. The action onsets in 15 minutes with peak actions in 30 to 90 minutes. Short acting insulin action onsets within 30 minutes with the peak action around 2 to 4 hours. Intermediate acting insulin action onsets within one to two hours with peak action of four to 10 hours. Long-acting insulin is usually given once per day. The action onset is roughly 1 to 2 hours with a sustained action of up to 24 hours. Some insulins are biosynthetic products produced using genetic recombination techniques; formerly, cattle or pig insulins were used, and even sometimes insulin from fish.
People with type 1 diabetes always need to use insulin, but treatment can lead to low BG (hypoglycemia), i.e. BG less than 70 mg/dl (3.9 mmol/l). Hypoglycemia is a very common occurrence in people with diabetes, usually the result of a mismatch in the balance among insulin, food and physical activity. Symptoms include excess sweating, excessive hunger, fainting, fatigue, lightheadedness and shakiness. Mild cases are self-treated by eating or drinking something high in sugar. Severe cases can lead to unconsciousness and are treated with intravenous glucose or injections with glucagon. Continuous glucose monitors can alert patients to the presence of dangerously high or low blood sugar levels, but technical issues have limited the effect these devices have had on clinical practice.
As of 2016 an artificial pancreas looks promising with safety issues still being studied.
Pancreas transplantation
In some cases, a pancreas transplant can restore proper glucose regulation. However, the surgery and accompanying immunosuppression required may be more dangerous than continued insulin replacement therapy, so is generally only used with or some time after a kidney transplant. One reason for this is that introducing a new kidney requires taking immunosuppressive drugs such as cyclosporine, which allows the introduction of a new pancreas to a person with diabetes without any additional immunosuppressive therapy. However, pancreas transplants alone may be beneficial in people with extremely labile type 1 diabetes mellitus.
Islet cell transplantation
Islet cell transplantation may be an option for some people with type 1 diabetes that are not well controlled with insulin. Difficulties include finding donors that are a compatible, getting the new islets to survive, and the side effects from the medications used to prevent rejection. Success rates, defined as not needing insulin at 3 years follow the procedure occurred in 44% in on registry from 2010.
 & diabetic ketoacidosis (DKA ...")
Complications
Complications of poorly managed type 1 diabetes mellitus may include cardiovascular disease, diabetic neuropathy, and diabetic retinopathy, among others. However, cardiovascular disease as well as neuropathy may have an autoimmune basis, as well. Women with type 1 DM have a 40% higher risk of death as compared to men with type 1 DM. The life expectancy of an individual with type 1 diabetes is 11 years less for men and 13 years less for women.
Urinary tract infection
People with diabetes show an increased rate of urinary tract infection. The reason is bladder dysfunction that is more common in diabetics than in non-diabetics due to diabetic nephropathy. When present, nephropathy can cause a decrease in bladder sensation, which in turn, can cause increased residual urine, a risk factor for urinary tract infections.
Sexual dysfunction
Sexual dysfunction in diabetics is often a result of physical factors such as nerve damage and/or poor circulation, and psychological factors such as stress and/or depression caused by the demands of the disease.
Males
The most common sexual issues in diabetic males are problems with erections and ejaculation: "With diabetes, blood vessels supplying the penis's erectile tissue can get hard and narrow, preventing the adequate blood supply needed for a firm erection. The nerve damage caused by poor blood glucose control can also cause ejaculate to go into the bladder instead of through the penis during ejaculation, called retrograde ejaculation. When this happens, semen leaves the body in the urine." Another cause for erectile dysfunction are the reactive oxygen species created as a result of the disease. Antioxidants can be used to help combat this.
Females
While there is less material on the correlation between diabetes and female sexual dysfunction than male sexual dysfunction, studies have shown there to be a significant prevalence of sexual problems in diabetic women. Common problems include reduced sensation in the genitals, dryness, difficulty/inability to orgasm, pain during sex, and decreased libido. In some cases diabetes has been shown to decrease oestrogen levels in females, which can affect vaginal lubrication.
Oral contraceptives can be taken by diabetics. Sometimes, contraceptive pills can cause a blood sugar imbalance, but this usually can be corrected by a dosage change. As with any medication, side effects should be taken into account and monitored to prevent serious complications with diabetes.
Women with type 1 diabetes show a higher than normal rate of polycystic ovarian syndrome (PCOS). The reason may be that the ovaries are exposed to high insulin concentrations since women with type 1 diabetes can have frequent hyperglycemia.

Epidemiology
Type 1 diabetes makes up an estimated 5-10% of all diabetes cases or 11-22 million worldwide. In 2006 it affected 440,000 children under 14 years of age and was the primary cause of diabetes in those less than 10 years of age. The incidence of type 1 diabetes has been increasing by about 3% per year.
Rates vary widely by country. In Finland, the incidence is a high of 57 per 100,000 per year, in Japan and China a low of 1 to 3 per 100,000 per year, and in Northern Europe and the U.S., an intermediate of 8 to 17 per 100,000 per year.
In the United States, type 1 diabetes affected about 208,000 youths under the age of 20 in 2015. Over 18,000 youths are diagnosed with Type 1 diabetes every year. Every year about 234,051 Americans die due to diabetes (type I or II) or diabetes-related complications, with 69,071 having it as the primary cause of death.

History
Type 1 diabetes was described as an autoimmune disease in the 1970s, based on observations that autoantibodies against islets were discovered in diabetics with other autoimmune deficiencies. It was also shown in the 1980s that immunosuppressive therapies could slow disease progression, further supporting the idea that type 1 diabetes is an autoimmune disorder. The name juvenile diabetes was used earlier as it often first is diagnosed in childhood.
In Australia, approximately one million Australians have been diagnosed with type 1 diabetes and Australia ranks 7th-highest in the world with children under 14 years of age. Between 2000 and 2013, 31,895 new cases were established, with 2,323 in 2013, a rate of 10-13 cases per 100,00 people each year. Aboriginals and Torres Strait Islander people are less affected.

Society and culture
The disease was estimated to cause $10.5 billion in annual medical costs ($875 per month per diabetic) and an additional $4.4 billion in indirect costs ($366 per month per person with diabetes) in the U.S. In the United States $245 billion every year is attributed to diabetes. Individuals diagnosed with diabetes have 2.3 times the health care costs as individuals who do not have diabetes. One in 10 health care dollars are spent on individuals with diabetes.

Research
Funding for research into type 1 diabetes originates from government, industry (e.g., pharmaceutical companies), and charitable organizations. Government funding in the United States is distributed via the National Institute of Health, and in the UK via the National Institute for Health Research or the Medical Research Council. JDRF, founded by parents of children with type 1 diabetes, is the world's largest provider of charity based funding for type 1 diabetes research. Other charities include the American Diabetes Association, Diabetes UK, Diabetes Research and Wellness Foundation, Diabetes Australia, the Canadian Diabetes Association.
A number of approaches have been explored to understand causes and provide treatments for type 1.
Diet
Data suggest that gliadin (a protein present in gluten) might play a role in the development of type 1 diabetes, but the mechanism is not fully understood. Increased intestinal permeability caused by gluten and the subsequent loss of intestinal barrier function, which allows the passage of pro-inflammatory substances into the blood, may induce the autoimmune response in genetically predisposed individuals to type 1 diabetes. There is evidence from experiments conducted in animal models that removal of gluten from the diet may prevent the onset type 1 diabetes but there has been conflicting research in humans.
Virus
One theory proposes that type 1 diabetes is a virus-triggered autoimmune response in which the immune system attacks virus-infected cells along with the beta cells in the pancreas. Several viruses have been implicated, including enteroviruses (especially coxsackievirus B), cytomegalovirus, Epstein-Barr virus, mumps virus, rubella virus and rotavirus, but to date there is no stringent evidence to support this hypothesis in humans. A 2011 systematic review and meta-analysis showed an association between enterovirus infections and type 1 diabetes, but other studies have shown that, rather than triggering an autoimmune process, enterovirus infections, as coxsackievirus B, could protect against onset and development of type 1 diabetes.
Stem cells
Pluripotent stem cells can be used to generate beta cells but previously these cells did not function as well as normal beta cells. In 2014 more mature beta cells were produced which released insulin in response to blood sugar when transplanted into mice. Before these techniques can be used in humans more evidence of safety and effectiveness is needed.
Vaccine
Vaccines to treat or prevent Type 1 diabetes are designed to induce immune tolerance to insulin or pancreatic beta cells. While Phase II clinical trials of a vaccine containing alum and recombinant GAD65, an autoantigen involved in type 1 diabetes, were promising, as of 2014 Phase III had failed. As of 2014, other approaches, such as a DNA vaccine encoding proinsulin and a peptide fragment of insulin, were in early clinical development.

References

External links
- Diabetes mellitus type 1 at DMOZ
- Kids and Teens: Type 1 Diabetes at DMOZ
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) - Diabetes in America Textbook (PDFs)
- IDF Diabetes Atlas
- type 1 Diabetes at the American Diabetes Association
- Chamberlain, James J.; Kalyani, Rita Rastogi; Leal, Sandra; Rhinehart, Andrew S.; Shubrook, Jay H.; Skolnik, Neil; Herman, William H. (12 September 2017). "Treatment of Type 1 Diabetes: Synopsis of the 2017 American Diabetes Association Standards of Medical Care in Diabetes". Annals of Internal Medicine. doi:10.7326/M17-1259.
Source of article : Wikipedia
